Layering HA and PMMA Fillers: Why the Logic Is Flawed
Layering HA and PMMA Fillers: Why the Logic Is Flawed

Layering HA and PMMA Fillers: Why the Logic Is Flawed
Dr. Luis Casavantes | Avanti Derma ®
One of our patients recently arrived with a personally-researched plan: start with 6–10 cc of Voluma (a hyaluronic acid filler), let it settle, then six months later layer Linnea Safe (a PMMA-based permanent filler) on top. His reasoning: HA is reversible, so it could "prepare the tissue" and smooth any irregularities before committing to something permane
It is a logical-sounding strategy. It is also one that most experienced injectors would strongly advise against — and understanding why reveals important truths about how these two categories of filler actually work.
Two Materials, Two Incompatible Mechanisms
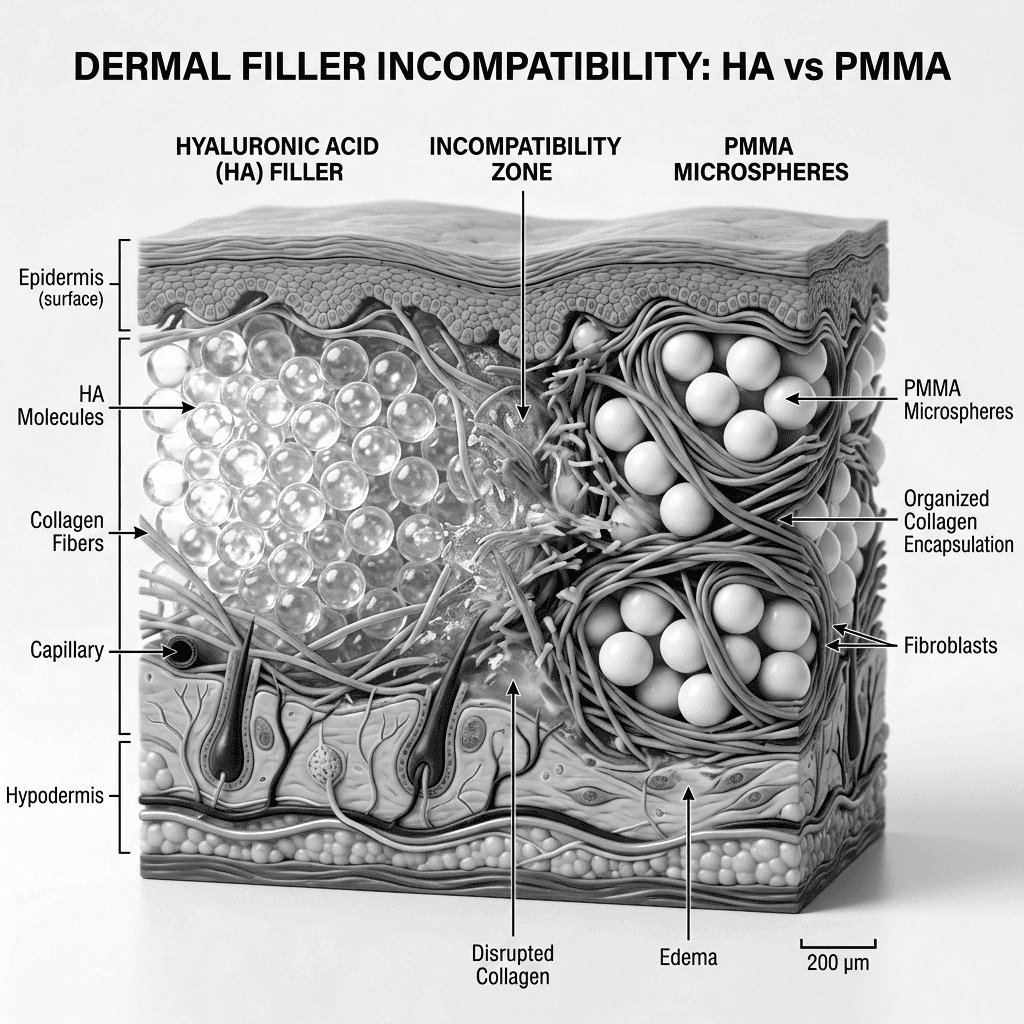
Hyaluronic acid is hydrophilic by nature — it actively absorbs and retains water, creating a fluid, hydrated microenvironment within the tissue planes where it is deposited. That is precisely what makes it effective as a volumizer, and precisely what makes it an unsuitable foundation for PMMA.
PMMA works through an entirely different biological process. Once injected, its smooth microspheres trigger a controlled foreign-body response: macrophages recognize the particles, fibrous tissue encapsulates them, and the resulting collagen matrix both preserves volume and anchors the microspheres permanently in place. This mechanism demands a stable, well-organized tissue environment — not one saturated with mobile, water-retaining HA.
Key risks of layering the two materials include:
Microsphere migration: PMMA microspheres may cluster or travel through the fluid pathways created by residual HA rather than distributing evenly.
Impaired encapsulation: The hydrated environment left by HA may disrupt the organized fibrotic response that PMMA depends on for permanence and structural integrity.
Irreversibility compounded by complexity: If a granuloma, seroma, or biofilm-related infection develops — risks documented with both material classes independently — the presence of two different foreign substances makes diagnosis and management significantly harder. HA can be dissolved with hyaluronidase; PMMA cannot be removed without surgery.
The Patient's Follow-Up — and Our Advice
When we explained this, the patient asked a thoughtful follow-up: would Ellansé (a biostimulatory filler with some reversibility) be a better intermediate step? The answer, in principle, is the same. The core problem is not which HA product precedes the PMMA — it is the act of layering materials with fundamentally different tissue interactions as a deliberate strategy.
"There is a consensus among most physicians to avoid mixing or overlapping different fillers, especially when their mechanisms of action are significantly different — as is the case with HA and PMMA." — Dr. Casavantes
Our recommendation is to choose one strategy from the outset. HA offers flexibility and reversibility; PMMA offers permanence. Both are valid choices — but they should be made cleanly, with a full consultation, rather than combined in a sequence that creates new risks without proportional benefit.
Clinical Takeaways
HA and PMMA operate through incompatible biological mechanisms and should not be deliberately layered.
PMMA depends on stable collagen encapsulation — a process that a prior HA environment may compromise.
Mixed-material complications are harder to diagnose and treat, particularly because PMMA is irreversible.
The safest path is selecting one filler strategy based on your goals and committing to it from the start.
Bibliography
Rzany, Berthold, and Hema Sundaram. "The Safety Profile of a Portfolio of Hyaluronic Acid-Based Soft Tissue Fillers Manufactured Using MACRO Technology: A Systematic Review of Clinical Evidence." PMC / PubMed Central, 2025. https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC12842927/.
Casavantes, Luis. Girth Matters: A Comprehensive Guide to Nonsurgical Male Enhancement. Avanti Derma, 2022. ISBN 978-1-7374986-0-5.
Wang, H., D. Wu, C. Lo, et al. "Foreign Body Granulomas Reaction Related to Collagen Stimulatory Cosmetic Fillers: A Systematic Review." Journal of Cosmetic Dermatology 24, no. 10 (2025): e70459. https://doi.org/10.1111/jocd.70459.
Lemperle, Gottfried. "Background/Basic Science of Polymethylmethacrylate Fillers." Rejuvenation Resource, March 9, 2021. https://www.rejuvenationresource.com/articles/ background-science/background-basic-science-of-polymethylmethacrylate-fillers.
Hu, X., Y. Zhang, H. Qin, et al. "Biofilm Formation Is a Risk Factor for Late and Delayed Complications of Filler Injection." Frontiers in Microbiology 14 (2024): 1297948. https:// doi.org/10.3389/fmicb.2023.1297948.
Requena, Luis, and Heinz Kutzner. "Foreign Body Granulomas after the Use of Dermal Fillers: Pathophysiology, Clinical Appearance, Histologic Features, and Treatment." American Journal of Clinical Dermatology (2011). PMC4366708. https:// pmc.ncbi.nlm.nih.gov/articles/PMC4366708/.